
Two Gunshot Wounds
Dr. S. Amjad Hussain

Image source: unsplash
Nineteenth century France, as most of the Western world at the time of Vincent Van Gogh’s death in 1890, was beginning to understand applied physiology as it pertained to the practice of medicine and surgery. The germ theory of disease as described by Louis Pasteur in 1861, was now widely accepted. The introduction in 1870 of antisepsis by the French surgeon Lucas Championniere, had paved the way for surgery beyond the realm of hernias and amputations. In Vienna, Theodore Billroth (1829-1894) had already performed total laryngectomy in 1873 and gastric resection in 1888. But, operations on the thorax would wait another 25 years when surgeons would be able to enter the chest cavity without harming the patient.
The impetus came after WWI when the US Army established an Empyema Commission to investigate reasons for high incidence of infections in chest cavities after gunshot wounds to the thorax. The Commission’s investigation led to the understanding of the physiology of negative intrathoracic pressure and opened the way for surgery within the thorax. The key to this success was re-establishment of negative intrathoracic pressure by inserting a drainage tube in the pleural cavity and placing the outer end under a pail of water. This water seal drainage while allowing the escape of fluid and air from the pleural cavity, prevented the entry of outside air into the chest. At the end of an operation the chest cavity was hermetically sealed as was intended by nature.
Vincent Van Gogh was the famous post impressionist Dutch painter (1853-1890) who suffered from mental illness and in 1890 took his life with a revolver when he was staying at a boarding house in the town of Auvers-su-Oisa in France. After breakfast on July 27, 1890, he went to the wheat fields that he had recently been painting. After a short while he walked back to the house and told the inn keeper that he had shot himself. He was treated by a country doctor by the name of Paul-Ferdinand Gachet. Lacking the skills of a surgeon Dr. Gachet did not probe the wound for locating and retrieving the bullet, as was the custom. He opted to simply dress the wound and told the attendants that nothing much could be done.

Wheat Fields by Vincent Van Gogh courtesy of Toledo Museum of Arts
After breakfast on July 27, 1890, he went to the wheat fields that he had recently been painting. After a short while he walked back to the house and told the inn keeper that he had shot himself.
That day Van Gogh was well enough to take some nutrition and smoke his pipe. However his condition deteriorated and he died thirty hours after the injury.
The reluctance of Dr. Gachet, Van Gogh’s physician, in treating his patient aggressively is understandable. There was very little he could do under the circumstances. To search for the bullet by probing a wound had always been fraught with complications and even disasters. It is quite conceivable that the artist was able to survive two days precisely because of the inaction of his physician. Dr. Gachet could have hastened his patient’s demise by being more invasive and aggressive.
The artist most likely had a slow bleed in the pleural cavity from injured lung that in turn caused gradual collapse of the lung. That in turn lead to mediastinal shift and possible compromise of cardiovascular and respiratory systems. It is also quite conceivable that by placement of a simple chest tube his life could have been spared.
One hundred years after Van Gogh’s death, I found myself facing a similar dilemma in a remote mountainous region of northern Pakistan.
While on an expedition in the Hindu Kush Mountains of northern Pakistan in 1992, I was staying at a government rest house in the town of Chitral when an urgent request came for help. A public protest in the bazaar had turned violent resulting in exchange of gunfire between protesters and the police. A young man had been shot in the chest with an AK-47 assault rifle. The medical superintendent of the hospital, a classmate from my college days, came to ask for my help.
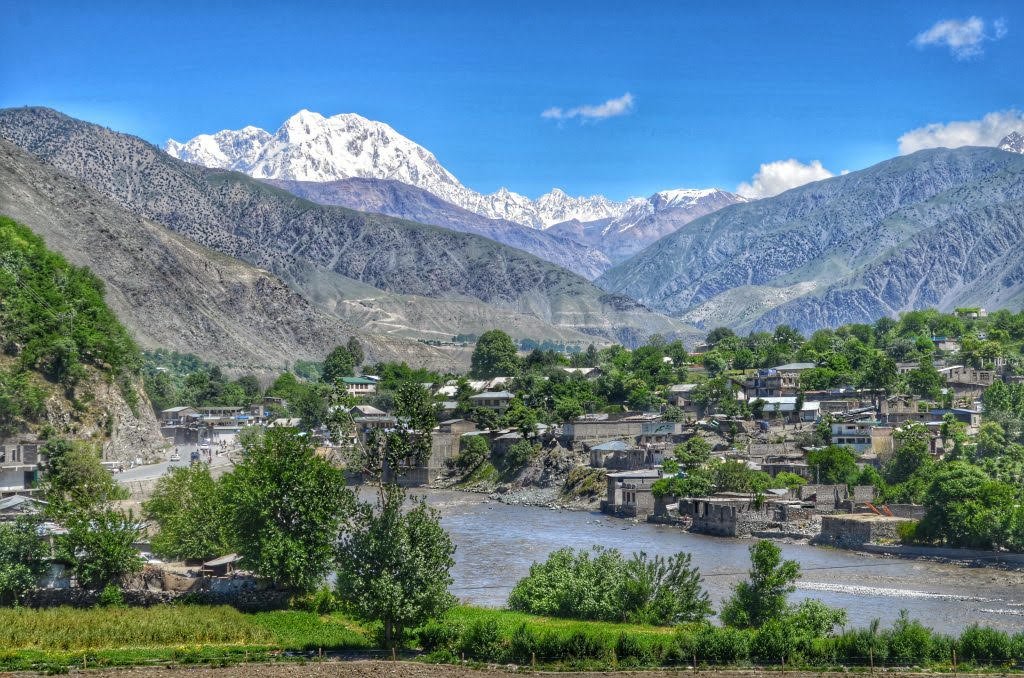
Town of Chitral in the Hindu Kush Mountains of Northers Pakistan.
The hospital was a spartan throw back from the days of the British Raj and lacked even the basic amenities. The young man, in his late teens, had a sucking wound on his right chest just below the nipple. He was extremely short of breath, had a low blood pressure and was coughing up bloody sputum. What the young man needed was replacement of his fast-depleting blood volume and insertion of a chest tube to help expand the collapsed lung. I ran in large quantities of intravenous fluids to stabilize the blood pressure and looked for a chest tube.
A search in the almost empty storeroom yielded an old red rubber flatus tube that probably had been used many times over for its intended purpose. Flatus tube is inserted through the anus into the colon to evacuate excess air from the colon. Lacking a proper chest tube, I opted to use the flatus tube after a good wash and sterilizing it in boiling water.
The tube and a few similarly sterilized instruments were taken to patient’s bedside. Without the niceties of local anesthesia, unavailable in any event, I inserted the tube in the right chest of the gasping young man and sutured the tube in place with a thick strand of silk. The other end of the tube was connected to a few feet of small caliber garden hose and the end of the hose was placed into a bucket of water. It could not get any more primitive.
There was a rapid drainage of considerable quantities of blood and air from the chest. Gradually his condition stabilized and after few hours the drainage decreased to a trickle and the air leak from the lung stopped. His breathing improved and he started to respond to his family and friends surrounding his bed.
When I visited him in the evening, he was sitting up in bed eating flat bread with sweetened milk tea. When asked how he was feeling, he said that the small incision I had made to insert the tube was more painful than the gunshot wound. I was later informed that he had made a full recovery.
There is a strange parallel between the dilemma Dr. Gachet faced a century earlier and the dilemma I faced in the Hindu Kush Mountains. We both were in the dark as to the exact nature of damage done to the structures in the chest. Dr. Gachet did not know what to do. I, on the other hand, was the recipient of the cumulative knowledge of medicine and surgery spanning the past century. But we both were helpless in different ways. I was lucky my patient did not have a lethal vascular or heart injury. A discarded flatus tube, a piece of garden hose and a bucket of water saved the day for both of us. Could they have done the same for Van Gogh if the knowledge and tools were available then? Perhaps.
Image Legend
1. Vincent Van Gogh self portrait
2. Vincent van Gogh (Dutch, 1853 – 1890), Wheat Fields with Reaper, Auvers, 1890, oil on canvas, 29 x 36 5/8 in. (73.6 x 93 cm).
3. Town of Chitral in the Hindu Kush Mountains of Northers Pakistan.

Dr. Sayed Amjad Hussain holds emeritus professorship in cardiothoracic surgery in the College of Medicine and Life Sciences and emeritus professorship in the College of Arts and Letters, University of Toledo. He has been an op-ed columnist for the Toledo Blade and essayist for The Friday Times of Lahore Pakistan. He is the author most recently of "A Tapestry of Medicine and Life".